It’s an exceedingly common and frustrating experience for patients to have tooth pain that seems to spread, radiate, and referral far beyond the actual tooth that’s diseased or damaged. This referred pain phenomenon can make it extremely challenging to accurately pinpoint which specific tooth is truly in need of dental treatment. So is it really possible for just one problematic tooth to generate perceived pain in several areas of the mouth? Let’s closely examine how dental pain referral works and the key mechanisms involved.
How dental pain referral happens

Tooth pain signals originate in the mouth before being transmitted to the brain for processing via the trigeminal nerve, which is the largest cranial nerve located in the head. This nerve contains three major sensory branches that convey pain signals originating from structures in the facial region, mouth, teeth, and lower jaw up to the central nervous system.
The three divisions of the trigeminal nerve each supply sensation to distinct areas:
- Ophthalmic division – Carries sensory axons from the eyes, forehead, and maxillary sinus regions.
- Maxillary division – Carries sensory axons from the upper jaw, upper teeth, nose, nasopharynx, and maxillary sinuses.
- Mandibular division – Carries sensory axons from the lower jaw, lower teeth, ear, temporomandibular joint, and posterior 1/3 of the tongue.
Within each nerve division, the peripheral axons transmitting pain information from the teeth are not isolated to just single teeth. The axons intersect, overlap, cross over, and crisscross to a significant extent, especially within the same trigeminal division.
This means a pain signal originating from one problematic molar or premolar, for example, can end up intersecting and crossing over with axons from neighboring molar and premolar teeth located nearby within the same division.
Due to this crossover, the brain struggles to precisely pinpoint which specific tooth initiation point is the true culprit for the pain. This phenomenon is referred to as dental pain referral or odontogenic pain referral. The perceived pain gets referred by the brain from the actual source tooth to other secondary sites along the same trigeminal nerve branch.
Common dental referral pain patterns
While dental pain referral can potentially radiate to any area innervated by the trigeminal nerve, there are some typical patterns that dentists watch for to aid in diagnosis:
Maxillary tooth referral pain patterns
- Maxillary central incisors – Typical referral pain sites involve the nasal region, nostril, and upper lip on the same side as the affected incisor.
- Maxillary lateral incisor – Common referral pain regions include the cheek, side of nose, upper lip, and maxillary sinus on the same side.
- Maxillary canines – Frequent referral pain areas involve the cheek, lower eyelid, side of nose, upper lip, and maxillary sinus on the same half of the face.
- Maxillary premolars – Common referral pain zones involve the cheek, temples, ear, maxillary sinus, and sometimes upper neck on the same side.
- Maxillary molars – Typical referral pain sites involve the cheek, temples, ear, temporomandibular joint, maxillary sinus, and possibly upper neck on the same side.
Mandibular tooth referral pain patterns
- Mandibular central incisors – Common referral pain locations involve the chin, lower lip, and anterior 2/3 of tongue on the same side.
- Mandibular lateral incisor – Typical referral areas include the chin, lower lip, anterior 2/3 of tongue, and inner cheek on the same side.
- Mandibular canines – Frequent referral sites involve the chin, lower lip, anterior 2/3 of tongue, inner cheek region, and temporomandibular joint on the same side.
- Mandibular premolars – Common referral pain regions include the cheek, temporomandibular joint, ear, temple, lower lip, tongue, and inner cheek on the affected side.
- Mandibular molars – Typical referral pain areas include the cheek, temporomandibular joint, ear, temple, posterior 1/3 of tongue, inner cheek, and jaw on the same side.
Common culprit teeth causing referred pain

While any tooth can generate and refer pain, third molars (wisdom teeth) and mandibular premolars are frequent offenders.
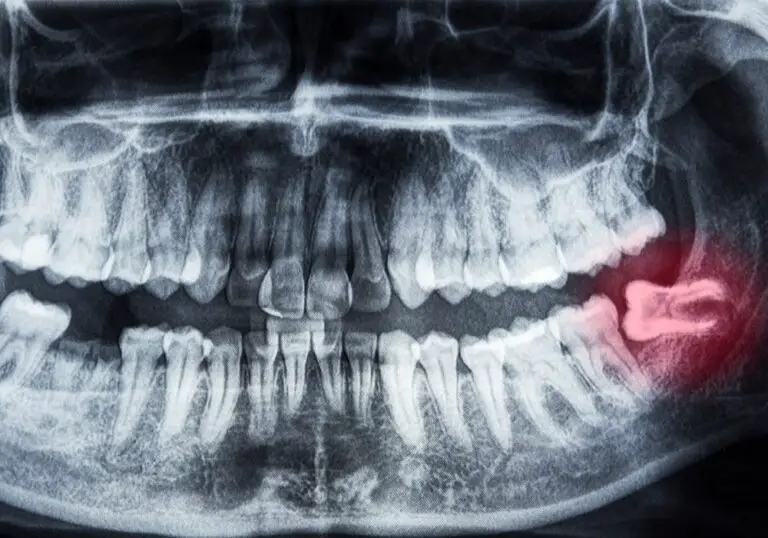
Wisdom teeth
Wisdom teeth are situated very far back in the mouth in the area around many other key anatomical structures. The nerve supply of third molars can intersect and cross over with nerves originating from the ear, maxillary sinus, posterior tongue, and temporomandibular joint.
As a result, it is quite common for pathologic issues with wisdom teeth to result in referral pain that radiates to the ear, sinus, tongue, TMJ, and surrounding jawline. The patient experiences these pains but cannot precisely pinpoint the third molar as the cause.
Mandibular premolars
The mandibular premolar teeth have overlapping and intersecting nerve innervation with the mandibular molars. Decay, damage, or other pathology involving a lower premolar often generates referral pain that seems to originate from the molars or general surrounding jaw joint instead.
Other potential causes of dental referral pain
While dental causes are the most frequent source, other trigeminal pathology can generate referred symptoms that feel like dental pain originating from the teeth:
- Temporomandibular joint disorders – Internal derangements and arthritic conditions involving the jaw joints often refer pain to the teeth, ears, temples, and back of the head.
- Trigeminal neuralgia – This chronic nerve pain disorder produces severe facial pain, often triggered by actions like brushing teeth or eating. Pain is referred along trigeminal nerve branches.
- Maxillary sinus infections – Congestion and inflammation of the maxillary sinuses can refer pain to the upper molars and jaw – even without actual dental issues.
- Myocardial infarction – In some patients, ischemic cardiac chest pain from heart attacks will radiate up into the jaw.
- Intracranial aneurysm – A burst cerebral aneurysm near cranial nerve roots can initially cause referred pain to the teeth before other neurological symptoms develop.
Diagnosing the precise source tooth

In order to determine which specific tooth is the definite origin of the dental referral pain, dentists will utilize a combination of approaches:
- Perform a very thorough clinical exam of all teeth, including periapical x-rays to identify occult decay or damage. Look for cracks, broken restorations, tenderness to percussion, etc.
- Assess the patient’s bite alignment and occlusion for excessive forces on any teeth.
- Use cold stimuli, percussion, palpation, and bite tests to check individual teeth for sensitivity and pain response.
- Potentially order CBCT scans to check for hidden abscesses, cysts, or abnormal anatomy.
- Assess pulp vitality and nerve health in the area via electric pulp or thermal heat/cold sensibility testing.
- Inject local anesthetic nerve blocks to temporarily numb suspected problem areas – pain relief indicates likely source.
While dental referral patterns provide clues about the possible origin, the only way to definitively diagnose the culprit tooth is to directly treat it by repair or extraction – complete resolution confirms the source.
Treating referred dental pain
Initially, treatment will focus on fixing the source tooth identified through testing, which may involve:
- Fillings to treat decay and replace lost tooth structure
- Root canal therapy to remove inflamed or necrotic pulp tissue
- Crowns to protect and strengthen teeth with cracks, fractures, or broken cusps
- Surgical extractions for non-restorable teeth or problematic impactions
- Dental splint therapy for cracked teeth or trauma
- Bite adjustments and night guards for occlusal overload
Topical anesthetics, over-the-counter pain relievers, opioids, NSAIDs, and local anesthetic blocks can offer symptomatic relief. However, full and permanent resolution of all referred pain relies on successful treatment of the primary underlying dental issue – even if that tooth appears relatively normal on exam.
Referred pain that persists after successful dental treatment may require additional diagnostic workup to check for other potential sources like temporomandibular joint disorders, trigeminal neuralgia, or maxillary sinusitis.
Can referred dental pain seem to skip around?
Based on typical referral patterns, it would seem like pain from one problematic tooth should be fairly consistent in location. However, many patients report dental pain that feels like it skips around and moves from tooth to tooth.
There are several potential explanations for this phenomenon:
- Actual active decay or damage shifting around – New dental problems can develop in other teeth over time and become symptomatic.
- Misdiagnosis of the primary source tooth – The first tooth treated may not have been the true origin, and another active problem tooth was missed.
- Extensive nerve crossover – Dental axons crisscross substantially, so pains get mixed up in signaling.
- Chronic dental pain – Long-standing pain can lead to central sensitization and atypical referral patterns.
So while there is generally one primary source tooth, the extensive intersections between dental nerve pathways means the perceived pain localization can be fluid and difficult to pinpoint. The standard referral patterns simply provide a starting point to guide diagnosis.
Frequently asked questions about referred dental pain
Can a single bad tooth really cause pain that spreads to other teeth?
Yes, it’s extremely common for one diseased or damaged tooth to generate pain that referral and radiates to multiple other areas – other teeth, jaw, ear, temples, etc. This pain referral phenomenon happens due to substantial crossover between the sensory nerve axons supplying different regions. The brain struggles to precisely identify the exact source.
Is all dental pain referral?
No, sometimes dental pain is more localized and precisely matches up with clear clinical exam and x-ray findings of a problem in a particular tooth. However referral pain is very frequent, especially with posterior teeth like molars and wisdom teeth. Their nerve supply overlaps considerably, allowing signals to get mixed up.
If the pain is referred, how do dentists determine which tooth needs treatment?
Dentists utilize the common dental referral pain patterns to provide an initial diagnostic starting point. They thoroughly clinically examine all teeth in the possibly affected quadrants. Additional testing like x-rays, pulp vitality, and local anesthesia can further isolate the source. In many cases, definitive diagnosis only comes from directly treating the suspected tooth and verifying if that relieves all pain.
Is it possible for referral pain to spread from one side to the other?
It is uncommon, but possible in some cases. Most dental referral pain remains localized to the same side as the original tooth because it spreads along branches on that side. But some patients have atypical trigeminal nerve anatomy or chronic pain conditions that may allow dental referral pain to radiate to the opposite side. However, the same-side pattern is far more typical.
If a sinus infection refers pain to my teeth, do I still need dental work done?
You may not necessarily require dental treatment if the tooth pain is conclusively from a sinus infection and no actual dental issues exist. However, it’s crucial to thoroughly rule out underlying problems first, since sinus congestion can occasionally mask or mimic dental issues. A tooth could appear normal but still have occult disease. Getting the sinusitis treated offers short-term relief, but an asymptomatic dental problem could certainly flare up again after antibiotic treatment finishes.
Conclusion
While the phenomenon of referred dental pain can feel quite confusing and frustrating for both patients and dentists, it actually serves an important protective purpose. The trigeminal nerve branches are essentially alerting the brain that something is amiss and deserves attention in the oral cavity. This provides a key opportunity to have the dental issue properly diagnosed and treated before it escalates into a dental emergency like facial swelling or jaw fracture.
In summary, even if the dental pain jumps around and is difficult to pinpoint, view it as motivation to get a very thorough examination and identify the underlying origin tooth. Prompt diagnosis and successful treatment of the primary culprit will ultimately provide complete resolution of all referred symptoms – even if that tooth isn’t where the worst pain is perceived. Fixing problems early is critical to prevent much more serious and expensive dental issues down the road.