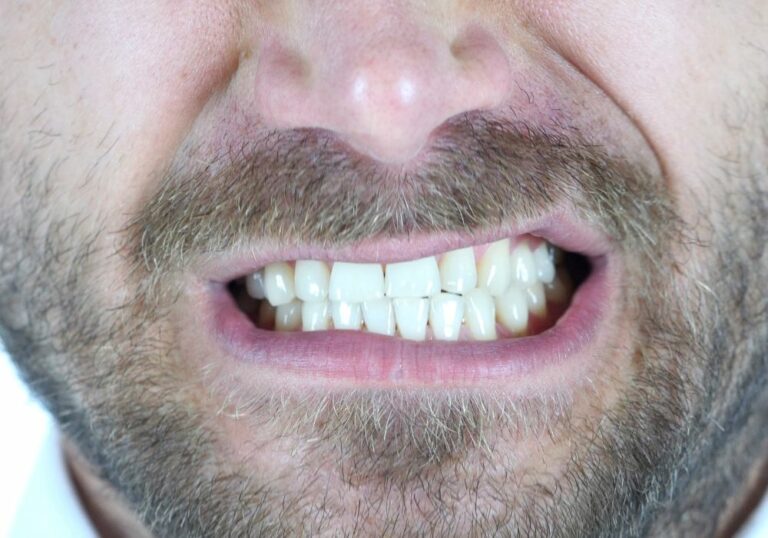
Tooth decay remains one of the most ubiquitous chronic diseases globally. Over 90% of adults worldwide have experienced cavities. In children, close to 60-90% have caries in their primary teeth. Untreated decay causes pain, infection, tooth loss, nutritional issues, and harm to quality of life.
Dental caries arises from a complex interplay of factors: susceptible teeth, cariogenic bacteria producing acids, and frequent exposure to fermentable carbohydrates. Once enamel is breached, decay spreads rapidly into the inner structures of the tooth. Preventing initial lesion development is key to maintaining oral health.
Fluoride plays an integral role in evidence-based caries management across the lifespan. Topical fluoride helps strengthen enamel against acidic attacks and promotes remineralization. It also inhibits the biofilm bacteria that initiate the caries process. Optimizing fluoride exposure is a pillar of preventive oral health.
A comprehensive history of fluoride and dental health

The use of fluoride for dental health began in the early 1900s. Scientists discovered high levels of naturally occurring fluoride in certain communities’ water sources. Residents in these areas surprisingly had lower rates of dental cavities, even without access to dental care.
Further investigation found fluoride made teeth more resistant to acid dissolution. Enamel crystals incorporated trace amounts of fluoride, protecting against decay. Scientists confirmed this by analyzing fluoride content in sound versus decayed enamel.
In the 1930s, four key epidemiological studies shone more light on fluoride’s effects. They compared cavity rates between cities with fluoride in water supplies versus cities without. The differences were striking – those exposed to 1ppm fluoride had 40-60% less decay. This compelling evidence spurred the initiation of community water fluoridation.
By 1945, the first city in the world – Grand Rapids, Michigan – began adding fluoride to its water supply. The famous 15-year Grand Rapids fluoridation study tracked its incredible impact – a 50-70% reduction in dental caries was observed in children. Several years later, Newburgh, New York implemented water fluoridation with similar success.
Over the next several decades, thousands of cities adopted artificial water fluoridation based on overwhelming positive findings. By the 1960s, studies shifted focus to topical fluoride applications like gels, rinses, and varnishes. Concentrated fluoride could be applied directly to teeth for maximum benefit.
Today with fluoridated water, fluoride toothpaste, and fluoride treatments, dental cavities have declined substantially. However tooth decay remains widespread, causing many lost school and work days and poor quality of life when untreated. Fluoride continues to be a key preventive tool for addressing this prevalent, chronic disease.
Themechanisms behind fluoride’s cavity-fighting effects
Decades of laboratory, animal, and human studies have illuminated how fluoride protects teeth:
Fluoride concentrates in the crystalline structure of developing enamel, making it more acid-resistant. It also gets incorporated into saliva and plaque fluid, providing ongoing topical contact with enamel.
Fluoride prevents demineralization, which is the dissolving of enamel minerals when acid is produced by cavity-causing bacteria. Fluoride helps prevent calcium and phosphate loss.
Fluoride also enhances remineralization, assisting with rebuilding and repairing microscopic areas of early decay. It does this by facilitating calcium and phosphate redeposition into porous lesions.
Fluoride inhibits enzymes in cariogenic bacteria that allow them to metabolize sugars and stick to teeth. With less biofilm formation and acid production, decay is hindered.
Modern research tools have shed light on fluoride’s anticarie mechanisms. However, scientists are still exploring the precise biochemical ways fluoride interacts with hydroxyapatite crystals in enamel and within dental plaque.
Identifying patients who can benefit from professional fluoride application

Due to its proven benefits, many patients are candidates for professional fluoride treatment in the dental office:
- Children and teens with a high past incidence of cavities. The goal is preventing future decay with concentrated fluoride.
- Patients with orthodontics like braces or aligners. Appliances retain food and promote high-risk areas around brackets.
- Patients with gum recession or exposed root surfaces. Root caries develop more easily without an enamel layer.
- Elderly patients, who often have gingival recession and lack dexterity for adequate home care.
- Patients with dry mouth conditions or taking medications that reduce salivary flow. Lack of saliva removes a key buffer against cavity acids.
- Patients with developmental conditions like autism who may be less cooperative with brushing. Fluoride provides an extra decay defense.
- Children or adults exposed to high-sugar diets. Dietary habits may be hard to break, so fluoride helps counteract acid attacks.
Identifying at-risk patients allows targeting of fluoride to those who need its cavity-preventive benefits the most.
The different professional topical fluoride options dentists have
Dentists have several types of professional fluoride treatments in their preventive arsenal:
Fluoride varnish – A resin-based, highly concentrated paste containing 5% sodium fluoride. Gentle drying and isolation of the teeth allows the varnish to set upon contact. It adheres to all tooth surfaces and provides sustained fluoride release. Varnish is quick and easy to apply, with minimal risk of ingestion.
Fluoride gels – A thicker gel containing 1.23% acidulated phosphate fluoride. Trays are filled with the gel and custom-fit to the patient’s teeth for 4 minutes of contact before spitting out. This allows higher concentrations of fluoride to bathe the teeth compared to foams or rinses.
Fluoride foam – A bubble gum-flavored dense foam dispensed from a pressurized canister. It contains 1.23% acidulated phosphate fluoride. The foam is dabbed onto teeth with a tray or disposable mouthpiece and left for 1-4 minutes before expectorating.
Fluoride rinse – A 0.05% sodium fluoride solution patients swish around in their mouth daily at home. Often prescribed for high-risk patients as an adjunct to professional treatments. Provides lower concentrations of fluoride but higher frequency of contact.
Silver diamine fluoride – An antimicrobial liquid containing silver and fluoride. It is highly effective at stopping active cavities from enlarging, especially helpful for patients unable to tolerate traditional fillings.
Professional products have much higher fluoride concentrations and sustained contact compared to over-the-counter pastes and rinses. This provides superior prevention and remineralization benefits to patients at elevated risk of caries.
Weighing the potential side effects of fluoride use

The risks of fluoride are negligible compared to its substantial benefits, but users should be aware of potential side effects:
- Dental fluorosis — This shows up as barely detectable white spots on enamel. It occurs only with chronic ingestion of excessive fluoride during tooth development. Careful use and spitting out pastes prevents fluorosis.
- Short-term tissue irritation — High concentrations may briefly irritate oral tissues, resolved by spitting and rinsing. Proper isolation during treatment prevents this.
- Ingestion upset — Accidentally swallowing high-dose fluoride may cause temporary nausea or vomiting. Suctioning and rinsing minimizes ingestion.
- Allergic reactions — Extremely rare given how commonly used and well-tolerated fluoride is. Discontinue if any hypersensitivity occurs.
- Fluoride toxicity — Acute toxicity requires intake of extremely high levels of fluoride, far above appropriate use. Fluoride is safe when directions for use are followed.
While these potential effects should be minimized with proper technique, they are transitory and insignificant compared to fluoride’s lifelong oral health benefits.
Answers to frequently asked questions about fluoride
Is fluoride safe to ingest?
Yes, in the tiny amounts present in fluoridated water and toothpaste, fluoride is perfectly safe to ingest. These low levels are not close to being toxic. Fluoridated water contains 0.7 ppm fluoride, far below toxic concentrations.
Are there any proven negative health effects of fluoride?
Hundreds of studies over 70+ years have found no proven adverse medical outcomes from systemic fluoride at the miniscule levels used to prevent cavities. Its safety is confirmed by leading health organizations worldwide.
Should fluoride be avoided during pregnancy?
No, there is no reason to avoid optimally fluoridated water or dental products during pregnancy. Fluoride intake at recommended low levels is safe and provides protection against increased decay risk during pregnancy.
Does fluoride accumulate in the body long-term?
No, fluoride does not accumulate with regular low-level chronic exposure, such as drinking optimally fluoridated water. About 50% of ingested fluoride is excreted in urine within 24 hours. Fluoride incorporated into bones and teeth does not accumulate to harmful levels.
Should I use fluoride-free toothpaste?
Fluoride toothpaste provides invaluable cavity protection, offering a 20-40% reduction in caries versus non-fluoridated pastes. Fluoride is safe in the small pea-sized amount used on bristles. Fluoride’s oral health benefits far exceed the negligible risks.